Abstract
Abstract
There is increasing evidence that malaria is associated with blood groups. Thus, this study was to investigate the distribution of malaria parasitaemia in relation to blood groups among febrile patients who sought medical attention at a Nigerian Military Hospital, Jos, Plateau State, Nigeria. Thick and thin blood films were made from each blood sample, and blood groups were determined by a standard tube agglutination technique. Out of 246 blood samples examined, 172 (69.92%) were infected with malaria parasites, while 74 (30.08%) were not infected. There was a significant difference (p < 0.05) in the distribution of malaria parasitaemia in relation to blood groups. The malaria parasitaemia was highest in blood group O+ with 31.71%. There was no significant difference (p > 0.05) in malaria parasitaemia in relation to sex. Females had the highest malaria parasitaemia of 36.99%. Malaria parasitaemia in relation to age groups showed no significant difference (p > 0.05); however, the age group 41 years and above had the highest parasitaemia of 19.92%. There was a significant difference (p < 0.05) in malaria parasitaemia in relation to Plasmodium species. Plasmodium falciparum was the most occurring species (67.07%) among the patients with parasitaemia. Plasmodium falciparum and P. vivax were found to infect more females than males. There was a significant difference (p < 0.05) in the severity of malaria parasitaemia among the patients, with mild infection being the most common at 36.59%. This work revealed that both males and females of all blood groups are at risk of malaria; therefore, malaria prophylactic and therapeutic strategies should be directed at all patients without discrimination based on blood groups.
Figures
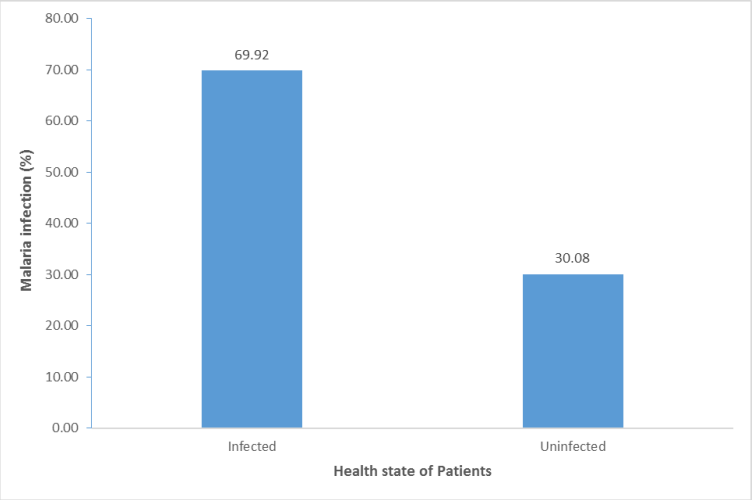
Figure 1: Malaria among patients attending Nigerian Military Hospital, Jos.
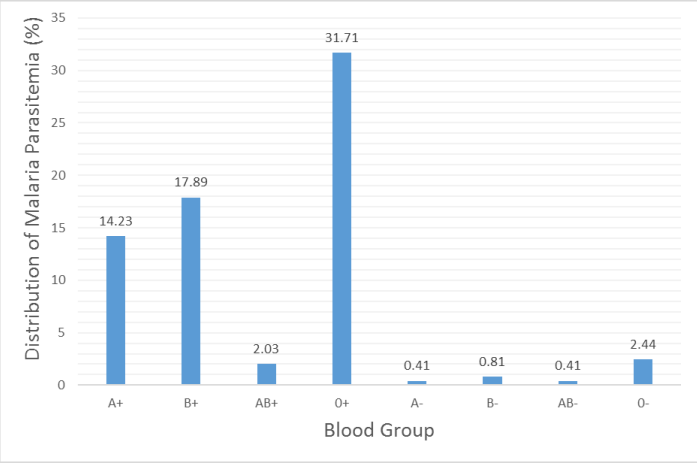
Figure 2: Distribution of malaria parasitaemia in relation to blood groups.
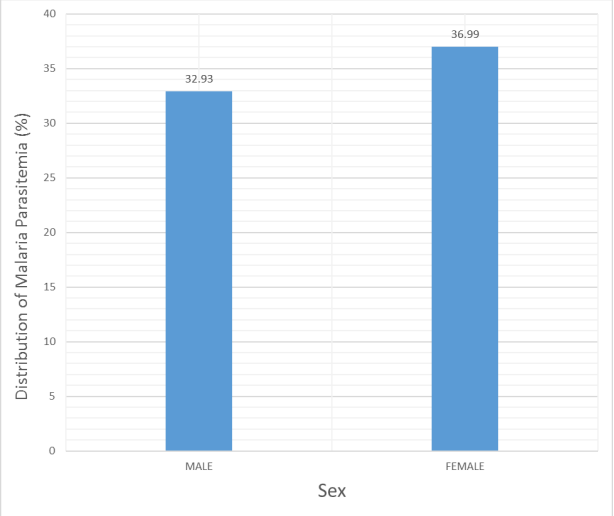
Figure3: Distribution of malaria parasitaemia in relation to Sex.
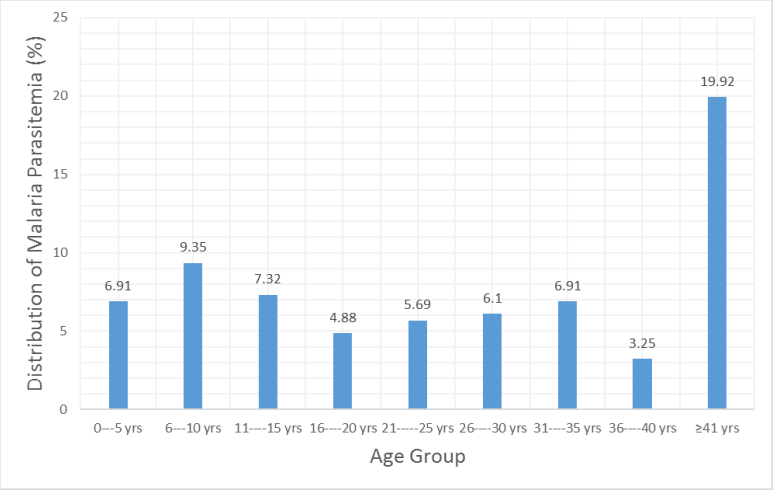
Figure 4: Distribution of malaria parasitaemia in relation to age groups.
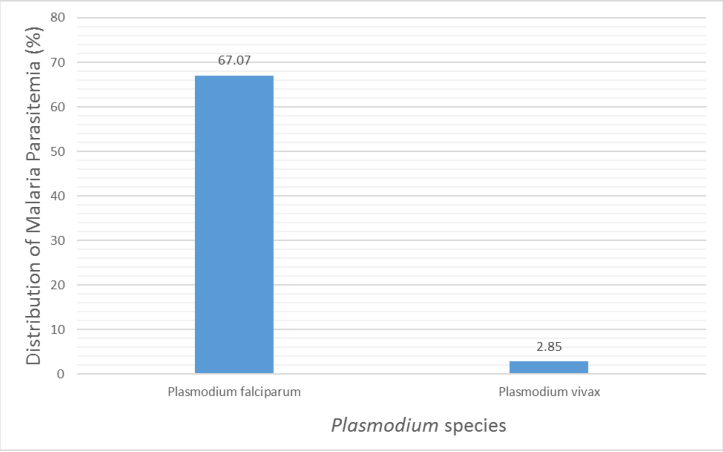
Figure 5: Distribution of malaria parasitaemia in relation to Plasmodium species.
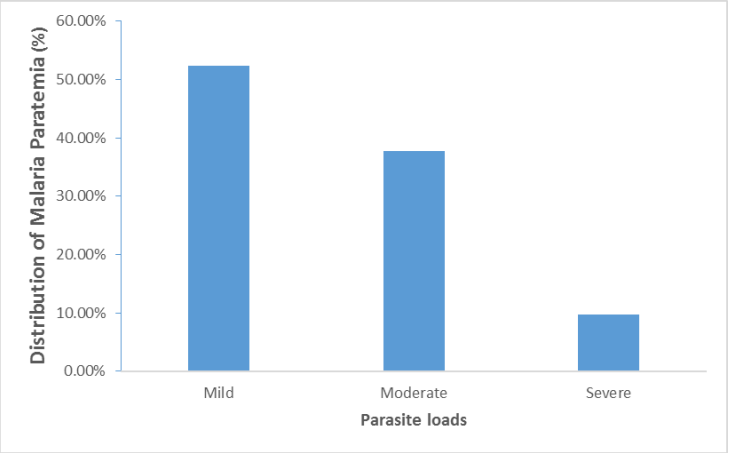
Figure 6: Distribution of malaria parasitaemia in relation to severity of the infection.
References
-
WHO. (2014) World Malaria Report 2008. Geneva: World Health Organization.
-
WHO. (2003) Prevention and control of Schistosomiasis and soil transmitted helminthiasis. World Health Organisation Technical Report Service. 912: 1–57.
-
Abeku TA. (2007) Response to malaria epidemics in Africa. Emerging Infectious Diseases. 14(5): 681–686.
-
Kwiatkowski DP. (2005) How malaria has affected the human genome and what human genetics can teach us about malaria. Am J Hum Genet. 77(2): 171–192.
-
Muntaka S, Opoku-Okrah C. (2013) The prevalence of malaria parasitaemia and predisposition of ABO blood groups to Plasmodium falciparum malaria among blood donors at a Ghanaian hospital. Department of Immunology, School of Molecular Medical Sciences, University of Nottingham, Nottingham, England, UK. African Union Journal of Technology. 16(4): 255–260.
-
Aliu SH, Onojo IS, Idoko T. (2014) Susceptibility of humans of the ABO blood groups to P. falciparum infection among patients attending Ahmadu Bello University Clinic (Sickbay), Samaru-Zaria, Kaduna State, Nigeria. Scholars Journal of Applied Medical Sciences. 2(40): 1305–1309.
-
Barragan A, Chen Q, Heddini A, et al. (2000) The semi-conserved head structure of Plasmodium falciparum erythrocyte membrane protein 1 mediates binding to multiple independent host receptors. J Exp Med. 192: 1–9.
-
Friedman J, Briand V, Watier L, et al. (1984) Coinfection with Plasmodium falciparum and Schistosoma haematobium: protective effect of schistosomiasis on malaria in Senegalese children. American Journal of Tropical Medicine and Hygiene. 72: 702–707.
-
Wolofsky V, Crompton PD, Pierce SK, et al. (2012) Advances and challenges in malaria vaccine development. Journal of Clinical Investigation. 120(12): 4168–4178.
-
Charan J, Biswas T. (2013) How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine. 35(2): 121–126.
-
Cheesebrough M. (2004) Medical Laboratory Manual for Tropical Countries (Volume II), Microbiology (Low Price Edition). Butterworth and Heinemann Ltd., Jordan Hill: 200–206.
-
WHO. (2005) Making every mother and child count. World Health Organization, Geneva. The World Health Report.
-
Atif SH, Farzana M, Naila S, et al. (2009) Incidence and pattern of malarial infection at a tertiary care hospital of Hyderabad. World Journal of Medical Sciences. 4(1): 9–12.
-
Ito EE, Egwunyenga AO, Ake JEG. (2014) Prevalence of malaria and human blood factors among patients in Ethiope East, Delta State, Nigeria. International Journal of Medicine and Biomedical Research. 3(3): 345–350.
-
Epidi TT, Nwani CD, Ugorji NP. (2008) Prevalence of malaria in blood donors in Abakaliki Metropolis, Nigeria. Scientific Research and Essay. 3: 162–164.
-
Rowe JA, Moulds JM, Newbold CI, et al. (1997) Plasmodium falciparum resetting mediated by parasite-variant erythrocyte membrane protein and complement-receptor 1. Nature. 388(6639): 292–295.
-
Vlassoff C, Bonilla A. (1994) Gender-related differences in the impact of tropical disease on women: What do we know? J Biosoc Sci. 26(1): 37–53.
-
Otajevwo FD. (2013) Prevalence of malaria parasitaemia and its association with ABO blood grouping among students of Igbinedion University, Okada, Nigeria. British Journal of Medicine & Medical Research. 3(4): 1164–1177.
-
Akanbi OM, Badaki JA, Adeniran OY, et al. (2010) Effect of blood group and demographic characteristics on malaria infection, oxidative stress and haemoglobin levels in South Western Nigeria. African Journal of Microbiology Research. 4(9): 877–880.
-
Bonilla E, Rodriguez A. (1993) Determining malaria effects in rural Colombia. Social Science and Medicine. 37(9): 109–114.
-
Ezenwelu UF. (1995) Prevalence of asymptomatic parasitaemia in an urban and rural community in south-western Nigeria. Central African Medicine. 41: 18–21.
-
Coker HAB, Chukwuani CM, Ifudu NO, et al. (2001) The malaria scourge concept in disease management. Journal of Pharmacy. 32: 19–49.
-
Nebe OJ, Adeboye GO, Agono PU. (2002) Prevalence and clinical profile of malaria among the coastal dwellers of Lagos State, Nigeria. Nigerian Journal of Parasitology. 23: 61–68.
-
Alli JA, Okonkwo IO, Abraham OA, et al. (2010) A serosurvey of blood parasites (Plasmodium, microfilariae, HIV, HBSAG, HCV antibodies) in prospective Nigerian blood donors. Research Journal of Medical Sciences. 4(4): 255–275.
-
Tidi SK, Amos JT, Firyanda E. (2013) Association between Plasmodium infection, haemoglobin genotypes and blood groups among under-five nomadic Fulani of Northeastern Nigeria. International Journal of Malaria Research and Reviews. 1(2): 7–11.
-
Brooks GF, Butel JS, Morse SA. (2004) Medical parasitology (23rd edn). The McGraw-Hill Companies, Inc., Boston: 818.
-
Singh G, Urheka AD, Singh R. (2015) A study on correlation of malaria infection with A, B, O, RH blood group system. Journal of Parasitology and Vector Biology. 7(4): 67–73.