1. Abstract
There is increasing evidence that malaria is associated with blood groups. Thus, this study was to investigate the distribution of malaria parasitaemia in relation to blood groups among febrile patients who sought medical attention at a Nigerian Military Hospital, Jos, Plateau State, Nigeria. Thick and thin blood films were made from each blood sample, and blood groups were determined by a standard tube agglutination technique. Out of 246 blood samples examined, 172 (69.92%) were infected with malaria parasites, while 74 (30.08%) were not infected. There was a significant difference (p < 0.05) in the distribution of malaria parasitaemia in relation to blood groups. The malaria parasitaemia was highest in blood group O+ with 31.71%. There was no significant difference (p > 0.05) in malaria parasitaemia in relation to sex. Females had the highest malaria parasitaemia of 36.99%. Malaria parasitaemia in relation to age groups showed no significant difference (p > 0.05); however, the age group 41 years and above had the highest parasitaemia of 19.92%. There was a significant difference (p < 0.05) in malaria parasitaemia in relation to Plasmodium species. Plasmodium falciparum was the most occurring species (67.07%) among the patients with parasitaemia. Plasmodium falciparum and P. vivax were found to infect more females than males. There was a significant difference (p < 0.05) in the severity of malaria parasitaemia among the patients, with mild infection being the most common at 36.59%. This work revealed that both males and females of all blood groups are at risk of malaria; therefore, malaria prophylactic and therapeutic strategies should be directed at all patients without discrimination based on blood groups.
2.Keywords:
Distribution, Malaria, Parasitaemia, Blood groups, Patients
3.Introduction:
Malaria is a life-threatening blood disease caused by the Plasmodium parasites and transmitted to humans by infected female Anopheles mosquito [1]. Malaria is said to be one of the world’s oldest diseases, which has often decimated populations with greater efficiency than wars [2]. The majority of malaria in Africa is caused by Plasmodium falciparum, which is the most dangerous of the human malarial parasites and is responsible for most of the mortality and morbidity associated with the disease. The interplay between malaria parasites and blood group antigens remains a fascinating subject with potential to contribute to the development of new interventions to reduce the global burden of malaria [2]. In 2013, 584,000 people globally died from malaria, with about 90% of the deaths occurring in Sub-Saharan Africa, where P. falciparum is the most prevalent parasite and the leading cause of malaria deaths [3]. Plasmodium falciparum has been called “the strongest known force for evolutionary selection in the recent history of the human genome” [4]. Its impact has been enormous, especially on children, where untreated cases have a 20-fold higher fatality rate than adults. Malaria, like other infectious diseases that kill children, selects for survival genes and prevents the transmission of genotypes unfavorable for survival. One such gene selected by malaria parasites is the ABO blood group gene, which has three alleles—A, B, and O—coding for different types of agglutinogens attached to the surface of red blood cells and determining an individual’s blood group [3]. The Plasmodium parasite has established a close relationship with red blood cells [5]. Severe pathophysiological manifestations of malaria caused by P. falciparum are a direct consequence of the parasite’s blood-stage replication cycle, during which merozoites repeatedly invade, multiply within, and destroy red blood cells. Consequently, red blood cells have evolved specific receptor-ligand interactions, some involving ABO blood group antigens, to facilitate adherence and invasion by merozoites [6]. Therefore, variations in erythrocyte ABO antigens can influence the penetration and establishment of merozoites. In terms of severity, P. falciparum is the most severe of the human malarial parasites [6]. There is strong epidemiological evidence that the ABO phenotype may modulate disease severity and outcomes of P. falciparum malaria, with blood groups A and B associated with increased severity compared to blood group O [7]. The Plasmodium parasite has been observed to have a reduced capacity to invade group O erythrocytes [8], while macrophages targeting P. falciparum-infected erythrocytes have been shown to clear infected O erythrocytes more effectively than infected A and B erythrocytes [9], indicating some level of resistance of blood group O to severe malaria.
4. Materials and Methods
4.1. The study area
The Military Hospital is located on Latitude 90 52’ 13” N and Longitude 80 53’ 30” E along plot 330, Ray field
road, Jos North LGA, Plateau State. The Military Hospital was established in the early 80’s.
4.2. Ethical clearance:
The study protocol was approved by the Military Hospital Ethical Review Committee before the commencement of the study.
4.3. Study population:
A total of 246 blood samples were considered for the study from patients across all age groups who sought medical attention at the Military Hospital. The sample size was estimated using the formula recommended by Charan & Biswas [10].
4.4. Consent of study population:
Before blood samples were collected, an explanation of the study was given, and written informed consent forms were issued to adult patients above 18 years of age, while assent forms were issued to the parents or guardians of children between the ages of 6–18 years to consent on their behalf.
4.5. Inclusion criteria:
Patients who were suspected to have malaria and were tested for malaria parasites using thick and thin film blood smear and microscopy.
4.6. Exclusion criteria:
Patients whose blood was not tested for malaria and febrile patients who had taken any antimalarial drugs within the last two weeks before the blood test were excluded, as well as those who did not consent or assent to the study.
4.7. Clinical and laboratory diagnosis of malaria parasites:
A total of 246 capillary blood samples were collected by finger pricking using a sterile disposable lancet for each patient after disinfecting the finger with 70% isopropanol; heel puncture was used for infants. Thick and thin blood films were immediately prepared, stained with 10% Giemsa for 15 minutes, washed in distilled water, and allowed to air dry. Examination of the films was carried out using an oil immersion objective (100x). For febrile patients who tested positive for Plasmodium parasites, the number of parasites (asexual forms only) was counted against 200 white blood cells (WBC) using hand tally counters, and the number of parasites per microliter was calculated.
4.8. Determination of blood groups:
Blood grouping was performed on each of the 246 blood samples using agglutination of antigens A, B, and D (Biotech Laboratories monoclonal, UK). Each blood sample was placed at three distinct spots on a slide on a white sterile tile; antigen A (blue), antigen B (yellow), and antigen D (colorless) were added and mixed using an applicator stick. The slides were then rocked for a few minutes to detect any agglutination, and the results were recorded appropriately [11]. 4.9. Statistical analyses: Data obtained were analyzed using R (Version 2.9.2). Proportions were compared using Pearson’s Chi-square test, and P-values < 0.05 were considered statistically significant.
5. Results
Out of 246 samples examined, 172 (69.92%) were infected with malaria parasites, while 74 (30.08%) were not infected (Figure 1). There was a significant difference (X² = 7.8015, df = 7, p < 0.001) in the distribution of malaria parasitaemia in relation to blood groups (Figure 2). The parasitaemia was highest in blood group O+ with 31.71%, while blood groups A− and AB− were the least, with occurrences of 0.41% each, as shown in Figure 2. There was no significant difference (X² = 1.9524, df = 1, p = 0.1623) in the distribution of malaria parasitaemia in relation to sex (Figure 3). Females had the highest parasitaemia rate of 36.99% compared to males with 32.93%. Similarly, the distribution of malaria parasitaemia in relation to age groups showed no significant difference (X² = 12.946, df = 8, p = 0.1137) as depicted in Figure 4. The age group 41 years and above had the highest parasitaemia rate of 19.92%, while 36–40 years had the least at 3.25% (Figure 4). There was a significant difference (X² = 145.14, df = 1, p < 0.001) in the distribution of malaria parasitaemia in relation to Plasmodium species (Figure 5). Out of the 172 patients infected with malaria parasites, 165 (67.07%) were infected with Plasmodium falciparum, while 7 (2.85%) were infected with Plasmodium vivax. Plasmodium falciparum was found to infect more females than males, at 35.37% and 31.71% respectively, while P. vivax showed a similar infection trend of 2.03% in females and 0.81% in males (Figure 5). There was a significant difference (X² = 48.012, df = 2, p < 0.001) in the severity of malaria among the patients (Figure 6). The mild level of infection was the highest at 36.59%, while the severe level was the least at 6.91%.
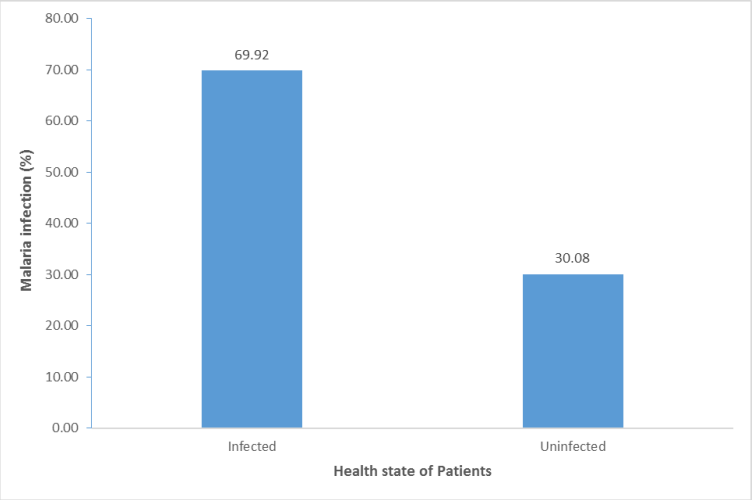
Figure 1: Malaria among patients attending Nigerian Military Hospital, Jos.
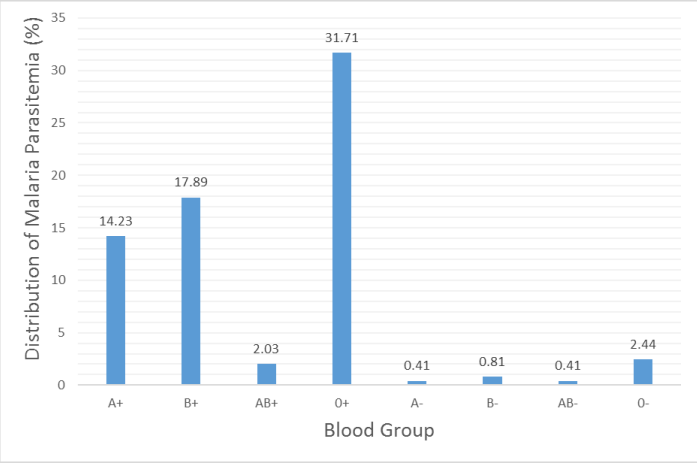
Figure 2: Distribution of malaria parasitaemia in relation to blood groups.
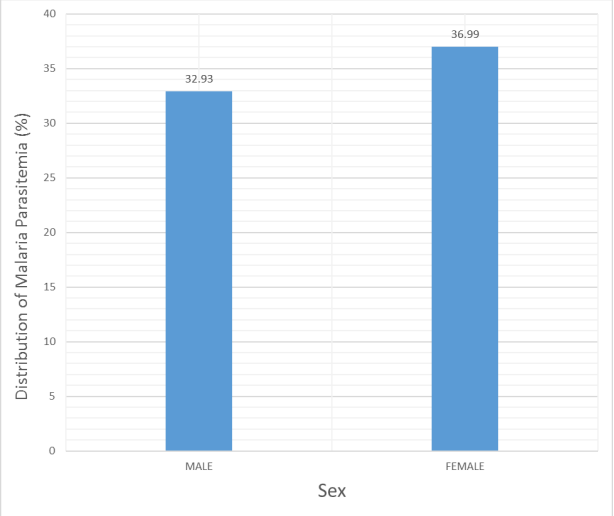
Figure3: Distribution of malaria parasitaemia in relation to Sex.
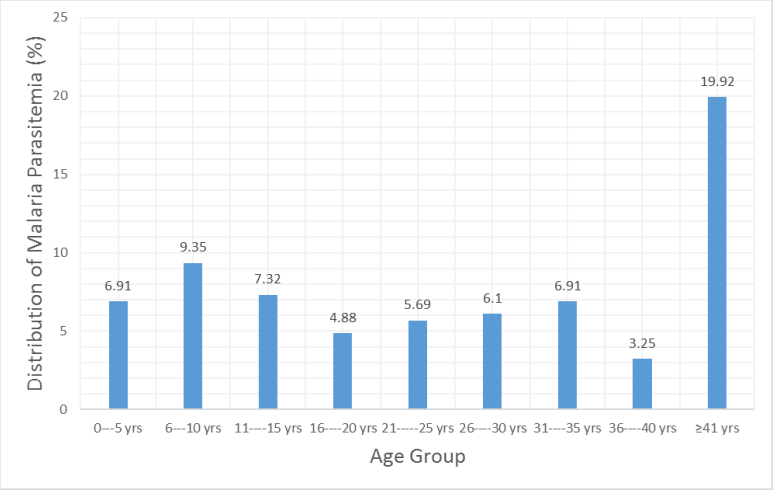
Figure 4: Distribution of malaria parasitaemia in relation to age groups.
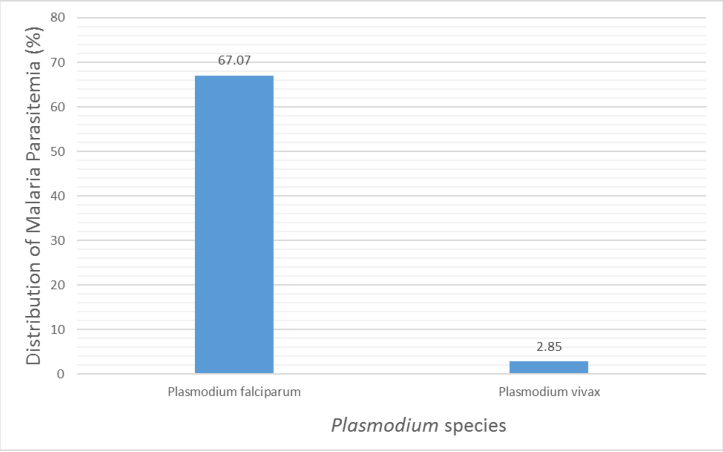
Figure 5: Distribution of malaria parasitaemia in relation to Plasmodium species.
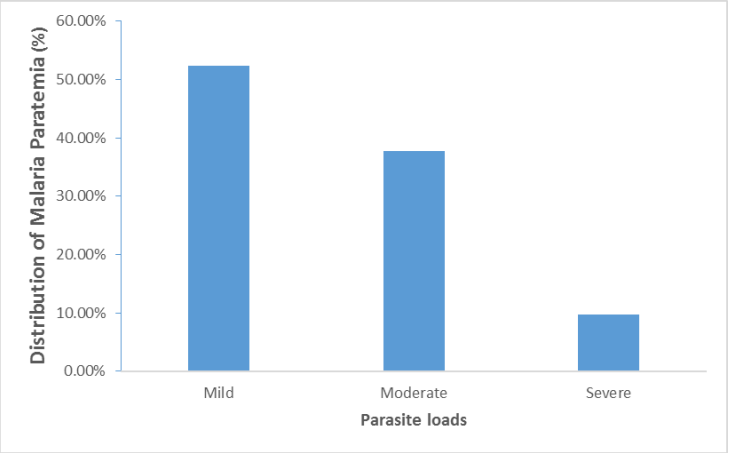
Figure 6: Distribution of malaria parasitaemia in relation to severity of the infection.
6. Discussion
Malaria accounts for 40% of public health expenditure, 30% of in-patient admission and up to 50% of outpatient visits in areas with high malaria transmission [12,13]. The overall prevalence of 69.92% reported in this study is lower compared to the overall prevalence of 83.98% reported by Ito, et al. [14] among patients in Ethiope East, Delta State, Nigeria. However, the overall prevalence in this study was higher compared to the overall prevalence of 51.5% reported by Epidi, et al. [15] among blood donors in Abakaliki, southeastern Nigeria. Malaria being highly prevalent in the patients attending a Nigerian Military hospital at this time can be attributed to the end of wet season, in which the bite of female Anopheles mosquitoes are at the peak. Though the raining season is almost ending, rains are usually at their peak in early October. During this period, water accumulates in gutters, pits, containers, abandoned tyres, leaves, and water reservoirs around homes, offices, market places and schools, create conducive breeding sites for malaria vectors. People living in close proximity to these breeding sites are more prone to bites from female Anopheles mosquitoes. It is evident that the patients who sought medical attention at the Nigerian Military Hospital, Jos come from areas with abundant breeding sites for mosquitoes. This study revealed that blood group 0+ significantly had the highest malaria parasitaemia compared to other blood groups. This observation is not surprising, as similar thing had been reported in other parts of Nigeria and other African countries. This corresponds with the report of Rowe, et al. [16] in Mali, where blood group O had the highest parasitaemia rate of uncomplicated malaria. This corresponds to the expected distribution of blood group O in malarious populations. Natural selection for resistance against malaria favours blood group O as it is protected against severe P. falciparum malaria, which is the most common in Africa [1]. Gender specific distribution of malaria parasitaemia showed that there was no significant difference between males and females patients. However, the distribution of malaria parasitemia was slightly higher in female. This correlates with the findings of Vlassoff and Bonilla [17] and [18] who reported that females are more infected than males. This high distribution of malaria parasitemia in females than males recorded in this work could be due to the fact that females expose their bodies more often than the males and thus increasing their chances of being bitten by the vectors [19].
The present study however, was in contrast to that of Bonilla and Rodriguez [20] and Muntaka and Opoku-Okrah [5] where males had a higher parasitaemia rate than females. This study also revealed that malaria parasitaemia could be age-related. A progressive increase in the distribution of the parasitaemia was observed as the age increases. This is consistent with the reports of some earlier studies in Nigeria [5,21,22]. The distribution of malaria parasitaemia was highest in the age group 41-years and above. This is in contrast with the findings of Nebe, et al. [23] who reported highest parasitaemia in adolescents. Alli, et al. [24] and Akanbi, et al. [19] reported that the degree of immunity is related to the duration of exposure to Plasmodium species which is longer for older persons. In this study Plasmodium falciparum was predominantly the species responsible for malaria. This is similar to the findings of Tidi, et al. [25]; Brooks, et al. [26] and Aliu, et al. [6]. The low prevalence of other Plasmodium species may be because they tend to be selective to the type of blood cells they infect. Plasmodium species infect red blood cells and young red blood cells than the old blood cells [27]. In this study, the mild cases of malaria infection were the highest followed by the moderate case and severe or chronic levels.
7. Conclusion and Recommendation
The prevalence of malaria in this study was 69.92%. The high prevalence of malaria parasitaemia encountered was due to socioeconomic factors, such as sanitary conditions, low standard of living, and inadequate use of insecticide treated nets in the study area. Both males and females with blood groups A, B, AB and O are equally at risk under any given circumstance. Consequently, administration of anti-malarial drugs (both prophylactic and therapeutic regimens) by Government and Non-Governmental health agencies should be directed at individuals of all groups without any discrimination or preference. Also, there is need for the government to incorporate control programs such as public enlightenment, free intensive distribution of insecticide treated nets (ITNs) and definitive diagnosis of malaria which will help to reduce the morbidity and mortality of the disease.
References
-
WHO. (2014) World Malaria Report 2008. Geneva: World Health Organization.
-
WHO. (2003) Prevention and control of Schistosomiasis and soil transmitted helminthiasis. World Health Organisation Technical Report Service. 912: 1–57.
-
Abeku TA. (2007) Response to malaria epidemics in Africa. Emerging Infectious Diseases. 14(5): 681–686.
-
Kwiatkowski DP. (2005) How malaria has affected the human genome and what human genetics can teach us about malaria. Am J Hum Genet. 77(2): 171–192.
-
Muntaka S, Opoku-Okrah C. (2013) The prevalence of malaria parasitaemia and predisposition of ABO blood groups to Plasmodium falciparum malaria among blood donors at a Ghanaian hospital. Department of Immunology, School of Molecular Medical Sciences, University of Nottingham, Nottingham, England, UK. African Union Journal of Technology. 16(4): 255–260.
-
Aliu SH, Onojo IS, Idoko T. (2014) Susceptibility of humans of the ABO blood groups to P. falciparum infection among patients attending Ahmadu Bello University Clinic (Sickbay), Samaru-Zaria, Kaduna State, Nigeria. Scholars Journal of Applied Medical Sciences. 2(40): 1305–1309.
-
Barragan A, Chen Q, Heddini A, et al. (2000) The semi-conserved head structure of Plasmodium falciparum erythrocyte membrane protein 1 mediates binding to multiple independent host receptors. J Exp Med. 192: 1–9.
-
Friedman J, Briand V, Watier L, et al. (1984) Coinfection with Plasmodium falciparum and Schistosoma haematobium: protective effect of schistosomiasis on malaria in Senegalese children. American Journal of Tropical Medicine and Hygiene. 72: 702–707.
-
Wolofsky V, Crompton PD, Pierce SK, et al. (2012) Advances and challenges in malaria vaccine development. Journal of Clinical Investigation. 120(12): 4168–4178.
-
Charan J, Biswas T. (2013) How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine. 35(2): 121–126.
-
Cheesebrough M. (2004) Medical Laboratory Manual for Tropical Countries (Volume II), Microbiology (Low Price Edition). Butterworth and Heinemann Ltd., Jordan Hill: 200–206.
-
WHO. (2005) Making every mother and child count. World Health Organization, Geneva. The World Health Report.
-
Atif SH, Farzana M, Naila S, et al. (2009) Incidence and pattern of malarial infection at a tertiary care hospital of Hyderabad. World Journal of Medical Sciences. 4(1): 9–12.
-
Ito EE, Egwunyenga AO, Ake JEG. (2014) Prevalence of malaria and human blood factors among patients in Ethiope East, Delta State, Nigeria. International Journal of Medicine and Biomedical Research. 3(3): 345–350.
-
Epidi TT, Nwani CD, Ugorji NP. (2008) Prevalence of malaria in blood donors in Abakaliki Metropolis, Nigeria. Scientific Research and Essay. 3: 162–164.
-
Rowe JA, Moulds JM, Newbold CI, et al. (1997) Plasmodium falciparum resetting mediated by parasite-variant erythrocyte membrane protein and complement-receptor 1. Nature. 388(6639): 292–295.
-
Vlassoff C, Bonilla A. (1994) Gender-related differences in the impact of tropical disease on women: What do we know? J Biosoc Sci. 26(1): 37–53.
-
Otajevwo FD. (2013) Prevalence of malaria parasitaemia and its association with ABO blood grouping among students of Igbinedion University, Okada, Nigeria. British Journal of Medicine & Medical Research. 3(4): 1164–1177.
-
Akanbi OM, Badaki JA, Adeniran OY, et al. (2010) Effect of blood group and demographic characteristics on malaria infection, oxidative stress and haemoglobin levels in South Western Nigeria. African Journal of Microbiology Research. 4(9): 877–880.
-
Bonilla E, Rodriguez A. (1993) Determining malaria effects in rural Colombia. Social Science and Medicine. 37(9): 109–114.
-
Ezenwelu UF. (1995) Prevalence of asymptomatic parasitaemia in an urban and rural community in south-western Nigeria. Central African Medicine. 41: 18–21.
-
Coker HAB, Chukwuani CM, Ifudu NO, et al. (2001) The malaria scourge concept in disease management. Journal of Pharmacy. 32: 19–49.
-
Nebe OJ, Adeboye GO, Agono PU. (2002) Prevalence and clinical profile of malaria among the coastal dwellers of Lagos State, Nigeria. Nigerian Journal of Parasitology. 23: 61–68.
-
Alli JA, Okonkwo IO, Abraham OA, et al. (2010) A serosurvey of blood parasites (Plasmodium, microfilariae, HIV, HBSAG, HCV antibodies) in prospective Nigerian blood donors. Research Journal of Medical Sciences. 4(4): 255–275.
-
Tidi SK, Amos JT, Firyanda E. (2013) Association between Plasmodium infection, haemoglobin genotypes and blood groups among under-five nomadic Fulani of Northeastern Nigeria. International Journal of Malaria Research and Reviews. 1(2): 7–11.
-
Brooks GF, Butel JS, Morse SA. (2004) Medical parasitology (23rd edn). The McGraw-Hill Companies, Inc., Boston: 818.
-
Singh G, Urheka AD, Singh R. (2015) A study on correlation of malaria infection with A, B, O, RH blood group system. Journal of Parasitology and Vector Biology. 7(4): 67–73.

Figure 1: Malaria among patients attending Nigerian Military Hospital, Jos.

Figure 2: Distribution of malaria parasitaemia in relation to blood groups.

Figure3: Distribution of malaria parasitaemia in relation to Sex.

Figure 4: Distribution of malaria parasitaemia in relation to age groups.

Figure 5: Distribution of malaria parasitaemia in relation to Plasmodium species.

Figure 6: Distribution of malaria parasitaemia in relation to severity of the infection.
-
WHO. (2014) World Malaria Report 2008. Geneva: World Health Organization.
-
WHO. (2003) Prevention and control of Schistosomiasis and soil transmitted helminthiasis. World Health Organisation Technical Report Service. 912: 1–57.
-
Abeku TA. (2007) Response to malaria epidemics in Africa. Emerging Infectious Diseases. 14(5): 681–686.
-
Kwiatkowski DP. (2005) How malaria has affected the human genome and what human genetics can teach us about malaria. Am J Hum Genet. 77(2): 171–192.
-
Muntaka S, Opoku-Okrah C. (2013) The prevalence of malaria parasitaemia and predisposition of ABO blood groups to Plasmodium falciparum malaria among blood donors at a Ghanaian hospital. Department of Immunology, School of Molecular Medical Sciences, University of Nottingham, Nottingham, England, UK. African Union Journal of Technology. 16(4): 255–260.
-
Aliu SH, Onojo IS, Idoko T. (2014) Susceptibility of humans of the ABO blood groups to P. falciparum infection among patients attending Ahmadu Bello University Clinic (Sickbay), Samaru-Zaria, Kaduna State, Nigeria. Scholars Journal of Applied Medical Sciences. 2(40): 1305–1309.
-
Barragan A, Chen Q, Heddini A, et al. (2000) The semi-conserved head structure of Plasmodium falciparum erythrocyte membrane protein 1 mediates binding to multiple independent host receptors. J Exp Med. 192: 1–9.
-
Friedman J, Briand V, Watier L, et al. (1984) Coinfection with Plasmodium falciparum and Schistosoma haematobium: protective effect of schistosomiasis on malaria in Senegalese children. American Journal of Tropical Medicine and Hygiene. 72: 702–707.
-
Wolofsky V, Crompton PD, Pierce SK, et al. (2012) Advances and challenges in malaria vaccine development. Journal of Clinical Investigation. 120(12): 4168–4178.
-
Charan J, Biswas T. (2013) How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine. 35(2): 121–126.
-
Cheesebrough M. (2004) Medical Laboratory Manual for Tropical Countries (Volume II), Microbiology (Low Price Edition). Butterworth and Heinemann Ltd., Jordan Hill: 200–206.
-
WHO. (2005) Making every mother and child count. World Health Organization, Geneva. The World Health Report.
-
Atif SH, Farzana M, Naila S, et al. (2009) Incidence and pattern of malarial infection at a tertiary care hospital of Hyderabad. World Journal of Medical Sciences. 4(1): 9–12.
-
Ito EE, Egwunyenga AO, Ake JEG. (2014) Prevalence of malaria and human blood factors among patients in Ethiope East, Delta State, Nigeria. International Journal of Medicine and Biomedical Research. 3(3): 345–350.
-
Epidi TT, Nwani CD, Ugorji NP. (2008) Prevalence of malaria in blood donors in Abakaliki Metropolis, Nigeria. Scientific Research and Essay. 3: 162–164.
-
Rowe JA, Moulds JM, Newbold CI, et al. (1997) Plasmodium falciparum resetting mediated by parasite-variant erythrocyte membrane protein and complement-receptor 1. Nature. 388(6639): 292–295.
-
Vlassoff C, Bonilla A. (1994) Gender-related differences in the impact of tropical disease on women: What do we know? J Biosoc Sci. 26(1): 37–53.
-
Otajevwo FD. (2013) Prevalence of malaria parasitaemia and its association with ABO blood grouping among students of Igbinedion University, Okada, Nigeria. British Journal of Medicine & Medical Research. 3(4): 1164–1177.
-
Akanbi OM, Badaki JA, Adeniran OY, et al. (2010) Effect of blood group and demographic characteristics on malaria infection, oxidative stress and haemoglobin levels in South Western Nigeria. African Journal of Microbiology Research. 4(9): 877–880.
-
Bonilla E, Rodriguez A. (1993) Determining malaria effects in rural Colombia. Social Science and Medicine. 37(9): 109–114.
-
Ezenwelu UF. (1995) Prevalence of asymptomatic parasitaemia in an urban and rural community in south-western Nigeria. Central African Medicine. 41: 18–21.
-
Coker HAB, Chukwuani CM, Ifudu NO, et al. (2001) The malaria scourge concept in disease management. Journal of Pharmacy. 32: 19–49.
-
Nebe OJ, Adeboye GO, Agono PU. (2002) Prevalence and clinical profile of malaria among the coastal dwellers of Lagos State, Nigeria. Nigerian Journal of Parasitology. 23: 61–68.
-
Alli JA, Okonkwo IO, Abraham OA, et al. (2010) A serosurvey of blood parasites (Plasmodium, microfilariae, HIV, HBSAG, HCV antibodies) in prospective Nigerian blood donors. Research Journal of Medical Sciences. 4(4): 255–275.
-
Tidi SK, Amos JT, Firyanda E. (2013) Association between Plasmodium infection, haemoglobin genotypes and blood groups among under-five nomadic Fulani of Northeastern Nigeria. International Journal of Malaria Research and Reviews. 1(2): 7–11.
-
Brooks GF, Butel JS, Morse SA. (2004) Medical parasitology (23rd edn). The McGraw-Hill Companies, Inc., Boston: 818.
-
Singh G, Urheka AD, Singh R. (2015) A study on correlation of malaria infection with A, B, O, RH blood group system. Journal of Parasitology and Vector Biology. 7(4): 67–73.